



Aortic valve replacement is a cardiac intervention performed to treat a failing aortic valve. This type of surgery is executed to replace a diseased valve. It can be degenerating because of different diseases, such as stenosis (narrowing) or regurgitation (leakage); it may be congenital (abnormal from birth) or an acquired disease (diseased with age). In either case, a malfunctioning aortic valve prevents blood from running normally in the heart’s chambers and therefore must be treated.
WHAT ARE THE SURGICAL OPTIONS?
- Mechanical valve — a long-lasting and durable valve which requires permanent oral anticoagulation therapy
- Valve made of tissue (more «natural» materials, which may include animal tissue)
- TAVI/TAVR procedure – The exact type is chosen based on the severity of symptoms and the potential surgical risks. In some cases, it is required that the patient takes intermediate medication in order to prevent blood clots creation.
Let’s focus on the TAVR/TAVI (Transcatheter Aortic Valve Replacement)/Transcatheter Aortic Valve Implantation), also known as Percutaneous Aortic Valve Replacement.
The TAVR is a technique used in the case of aortic stenosis. Every year the number of medical interventions using this procedure is growing. Usually, valve replacement requires an open heart procedure with a sternotomy; the chest is then surgically opened. The TAVR or TAVI procedure can also be done through very small openings in order to avoid a maximum move of the chest bones. As of now, this technique is reserved for elderly subjects or subjects showing surgical contraindication.
It’s also good to remind that the two valves used all around the world are French inventions! These are the two prostheses authorized in France for daily clinical use.

HISTORY OF AORTIC VALVE REPLACEMENT SURGERY:
The first implantation in a human body happened in 2002 in France. Since then, France has been the pioneer of TAVR and has been practicing it for a while now. TAVR had become a therapeutic reference regarding high surgical risk patients.
TAVR was approved by the American FDA in late 2011 for the treatment of people who have severe symptomatic aortic stenosis deemed inoperable. In August 2016, they finally extended the indications for patients with aortic valve stenosis who may undergo complications associated with open-heart surgery. These devices were previously approved only in patients at high or greater risk for death or complications during surgery.
The European, and more importantly, the French TAVR experience is longer with also, a broader selection of valves available to operators.

HOW A TAVR/TAVI PROCEDURE GOES:
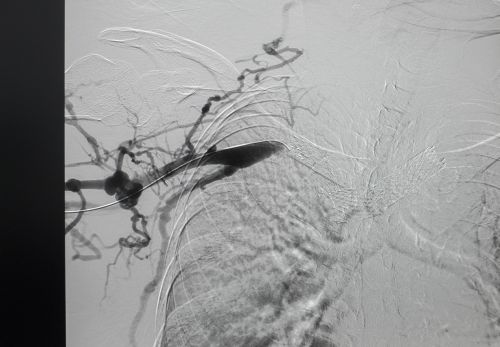
The implementation of these valves is preferably done by the percutaneous femoral route. However, hardware footprint causes that surgeons to regularly use alternative routes such as transaortic or carotid pathways. Surgical fellowships are established in advance; then the procedure is typically performed under angiographic control in a hybrid intervention room.
At the very beginning, the patient is given general or local anesthesia. Then the basic steps for a TAVR procedure goes as following:
- A medical doctor inserts a catheter (a hollow tube) that has a balloon at the tip into an artery, usually in the patient’s groin.
- Then, the catheter is passed into the patient’s heart and is positioned in the aortic valve opening.
- The doctor gently inflates the balloon in order to make room for the new tissue valve, which is placed in the position.
- The new valve can either expand by itself or is mechanically expanded using the balloon. The technique is chosen based on which type of valve material is used.
- The doctor deflates the balloon and removes all material.
- Now the patient has the new valve sitting inside their damaged valve.
HOW DOES RECOVERY GO?
Depending on the age and comorbidities of the patient, a journey back home can be considered within 3 days following the procedure. Generally, it takes about a month before full recovery, but it is very individual and can vary greatly.
THE FORTHCOMING OF THE TAVR PROCEDURE:
When considering the present results, extended indications are imminent even though ones’ recklessness is moderate by others’ common sense. The TAVR extension to intermediary risked subjects is already being considered in some European registers. Registers indicate that results for the concerned patients are as good, sometimes better than classical open-heart surgery. This extension should improve techniques, reduce serious complications and help understand material sustainability. Finally, the future may also bring new types of valves that are in their early stage of evaluation.
May 3rd, 2016, in Lyon, a patient was able to get an aortic valve replacement in an ambulatory way. The medical intervention lasted approximately an hour. The 86 years old patient was out 12 hours following his admission. It was a premiere in Europe!
If you’re in need of any type of aortic valve replacement, do not hesitate to contact us! We are able to get you the best treatments, by the best French surgeons!